Standard Use Procedures
Measurement protocols and functional examples for clinicians using the Splayometer for finger and hand extension and abduction strength assessment.
How to use these procedures
Following a consistent protocol is essential for obtaining reliable, comparable measurements across sessions and examiners.
Indications for Use
The Splayometer is indicated for quantitative assessment of voluntary finger and hand extension and abduction strength in adults. Intended use contexts include:
- Baseline hand strength assessment at the start of a course of care
- Serial measurement to monitor progress over time
- Bilateral comparison of affected versus unaffected hand
- Outcome documentation for clinical, insurance, or medico-legal purposes
Guiding Clinical Framework
Within the Occupational Therapy Practice Framework: Domain and Process (4th ed.; AOTA, 2020), hand strength assessment addresses client factors — specifically neuromusculoskeletal and movement-related body functions, including muscle power functions. These client factors underlie a client's ability to perform occupations such as activities of daily living (ADLs), instrumental activities of daily living (IADLs), work, and leisure.
Splayometer measurement is conducted as part of the occupational therapy evaluation process to analyze how finger extension and abduction strength contribute to or limit occupational performance. Results directly inform goal setting, intervention planning, and outcome measurement — all core elements of the OTPF-4 process. Because the OTPF-4 frames assessment holistically, clinicians should interpret Splayometer findings in context: alongside the client's occupational profile, environmental factors, and performance patterns (AOTA, 2020).
Standard Positioning Principles
Consistent positioning reduces examiner variability and ensures measurements are comparable across sessions. Because normative data for the Splayometer is still being developed, within-patient comparisons are currently more meaningful than reference to population norms. Replicating position exactly across sessions is therefore essential.
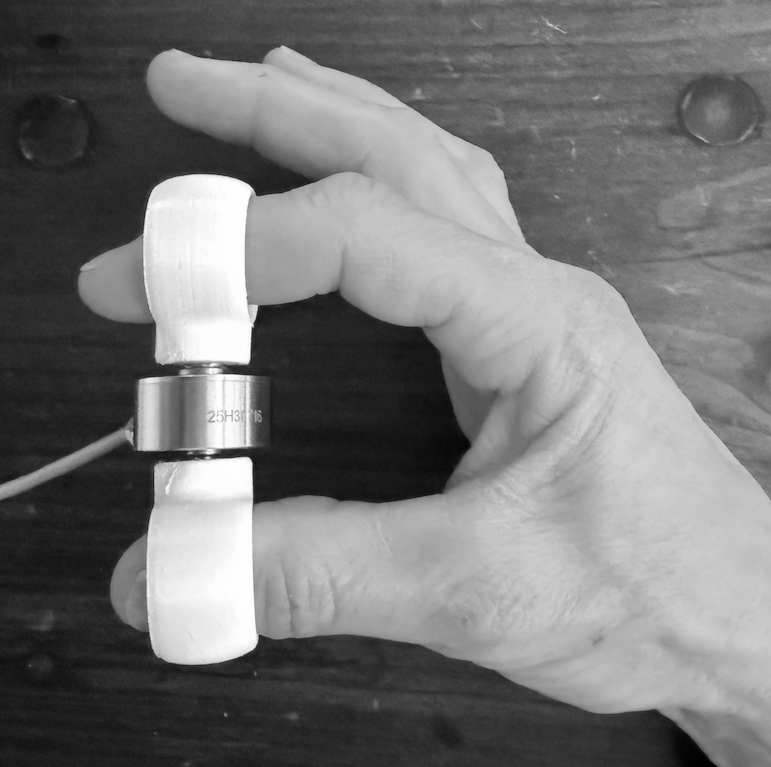
Finger-to-Thumb Extension
- Select finger rings sized for the target finger and for the thumb.
- Place one ring on the distal or middle phalanx of the target digit; place the second ring on the thumb. Ensure rings are seated comfortably and do not cause discomfort or restrict blood flow.
- Instruct the patient to extend the target finger away from the thumb — spreading the two rings apart — with maximum voluntary effort.
- Demonstrate the motion once if needed. Ensure the patient understands: they are extending, not flexing, and that motion should be smooth rather than jerky.
Test each digit of interest individually. Document which digit was tested (D1–D5) and which digit served as the anchor (typically thumb / D1).
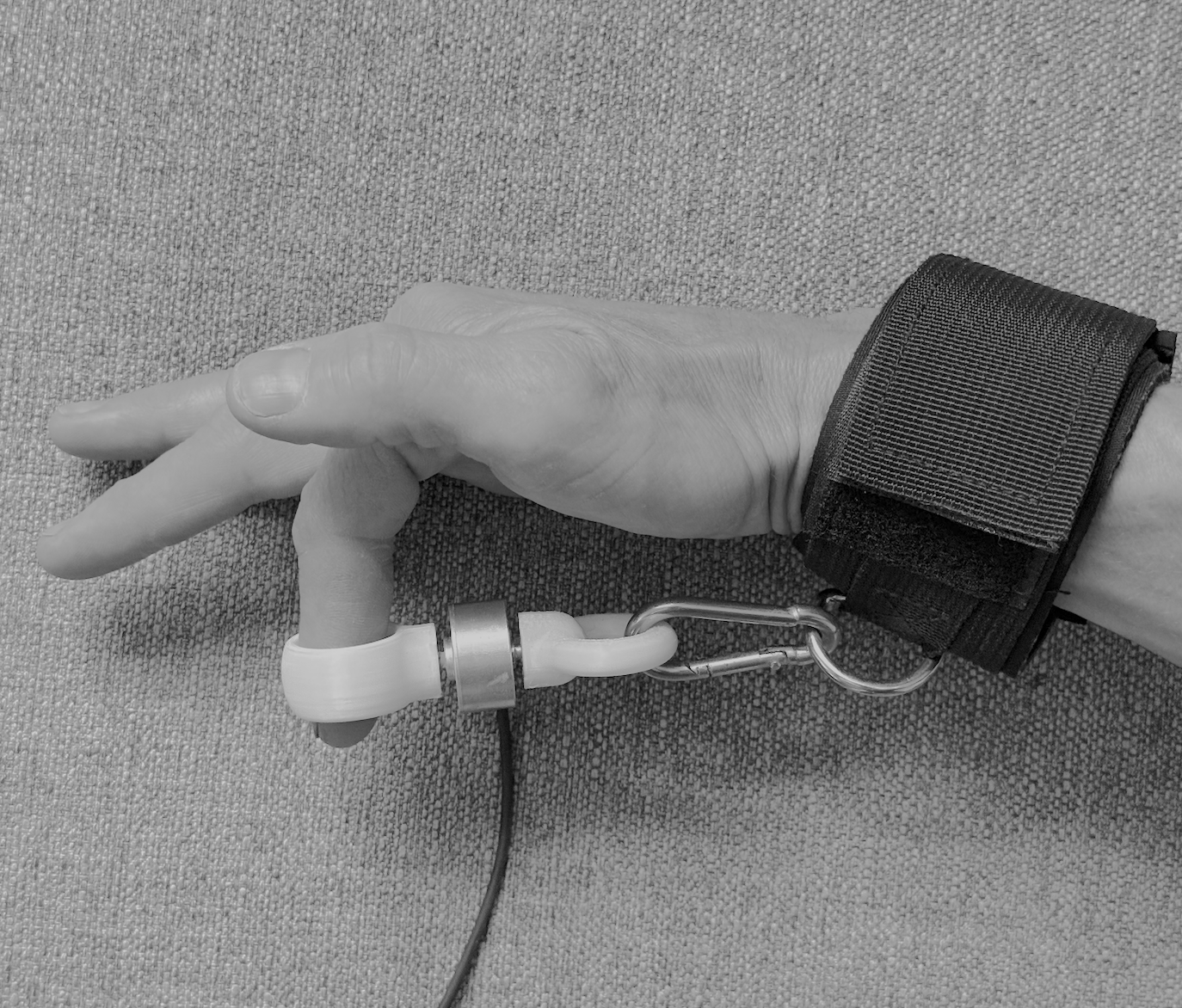
Finger-to-Hand Extension
- Select finger ring for the index, middle, ring or little finger.
- Connect wrist strap to hand, and connect to thin ring attachment.
- Instruct the patient to extend the finger away from the wrist with maximum voluntary effort.
Thumb extension and abduction may be clinically relevant in conditions such as de Quervain's tenosynovitis, CMC joint arthritis, or post-operative thumb reconstruction.
Hand Extension & Abduction
- Attach the hand loop to the load cell using the twist-lock connector.
- Position the loop over the dorsum of the four fingers (index through little). The loop should rest at approximately the level of the proximal phalanges. The thumb may be included or excluded — document which configuration is used and replicate it across sessions.
- Instruct the patient to open the hand — extending and spreading the fingers against the loop — with maximum voluntary effort.
Whole-hand measurement provides a composite of total hand opening force. It is a useful global indicator but does not isolate individual digit contributions. Use single-digit protocols where digit-specific data is required.

Finger-to-Thumb Pinch
- Select finger ring for the index, middle, ring or little finger.
- Connect wrist strap to hand, and connect to thin ring attachment.
- Instruct the patient to extend the finger away from the wrist with maximum voluntary effort.
Thumb extension and abduction may be clinically relevant in conditions such as de Quervain's tenosynovitis, CMC joint arthritis, or post-operative thumb reconstruction.

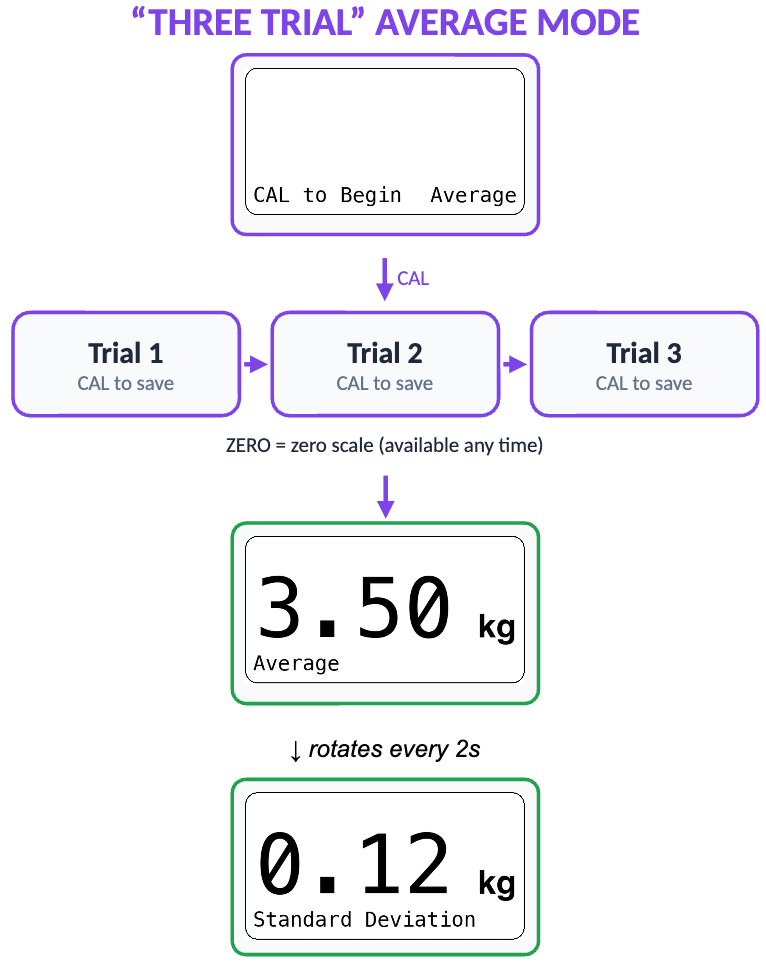
The Three-Trial Standard
A three-trial protocol is consistent with established dynamometry practice for grip and pinch and is recommended for all Splayometer measurements.
Instructions to the Patient
Before the first trial, instruct the patient clearly:
- "Push as hard as you can."
- "Keep pushing until I tell you to stop." (approximately 3 seconds)
- "Rest between each attempt."
Scoring
In Average mode, the Splayometer will record the peak force value for each of the three trials, and automatically computes the mean (average) and standard deviation of all three trials.
Rest Interval: 60 Seconds
A 2018 study (Kim et al.) found that three consecutive trials with a 60-second interval is the minimum optimal protocol for maximal handgrip strength measurement.
Order of Testing
Complete all trials for one hand before switching to the other. Test the unaffected or dominant hand first when possible to establish patient understanding of the task.
Bibliography
Sources supporting the protocols, clinical context, and recommendations described on this page.
- American Occupational Therapy Association. (2020). Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy, 74(Suppl. 2), 7412410010. https://doi.org/10.5014/ajot.2020.74S2001
- Coldham, F., Lewis, J., & Lee, H. (2006). The reliability of one vs. three grip trials in symptomatic and asymptomatic subjects. Journal of Hand Therapy, 19(3), 318–327. https://doi.org/10.1197/j.jht.2006.04.002
- Fess, E. E. (1992). Grip strength. In J. S. Casanova (Ed.), Clinical Assessment Recommendations (2nd ed., pp. 41–45). American Society of Hand Therapists.
- Kim, J. Y., Kwon, K. B., Song, S. H., Kwon, S.-S., Kang, B. Y., & Kim, D. H. (2018). Minimum optimal trials and interval during measurement of maximal handgrip strength. Isokinetics and Exercise Science, 26(3), 193–200. https://doi.org/10.3233/IES-171103
- Mathiowetz, V., Kashman, N., Volland, G., Weber, K., Dowe, M., & Rogers, S. (1985). Grip and pinch strength: Normative data for adults. Archives of Physical Medicine and Rehabilitation, 66(2), 69–74.
- Mathiowetz, V., Weber, K., Volland, G., & Kashman, N. (1984). Reliability and validity of grip and pinch strength evaluations. Journal of Hand Surgery, 9(2), 222–226. https://doi.org/10.1016/S0363-5023(84)80146-X
Looking for Normative Reference Values?
See references for grip, pinch, extension and abduction strength.